![]()
![]()
![]()







BONE TISSUE
PHYSIOLOGY:
The skeletal system has many functions. Among them are: support and
protection of the body, movement, blood formation, electrolyte and acid-base
balance, and detoxification.
ANATOMY
SHAPES AND GENERAL FEATURES OF BONES
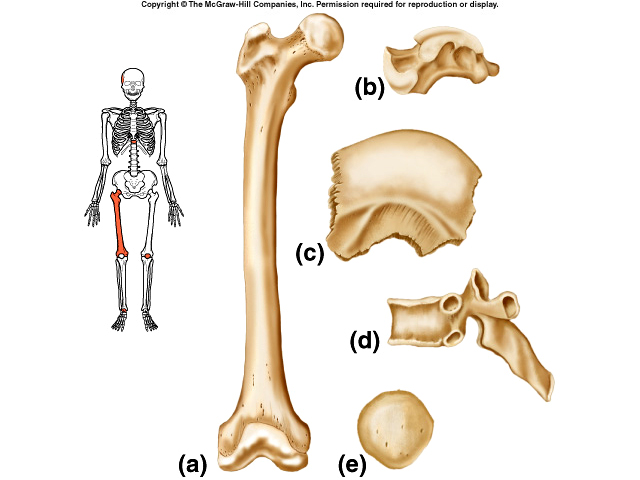 Long Bones (a) have greater length than width, consist of a shaft and a
variable number of extremities, are slightly curved for strength, consist
primarily of compact bone, but also contain much spongy bone and include bones
of the legs, arms, fingers and toes.
Long Bones (a) have greater length than width, consist of a shaft and a
variable number of extremities, are slightly curved for strength, consist
primarily of compact bone, but also contain much spongy bone and include bones
of the legs, arms, fingers and toes.
Short Bones (b) are somewhat club shaped, nearly equal in length and width, and consist of spongy bone except at the surface where there is compact bone. Examples are wrist and ankle bones.
Flat Bones (c) are generally thin and composed of two parallel plates of compact bone enclosing a layer of spongy bone. They offer considerable protection and provide extensive area for muscle attachment. Examples include cranial bones, sternum, ribs and shoulder blade.
Irregular Bones (d) have complex shapes and cannot be grouped into any of the other types. They vary in amount of compact and spongy bone present. They include backbone and certain facial bones.
The skeleton contains four types of connective tissue; periosteum,
cartilage, bone, and bone marrow. Other terms associated with bones are: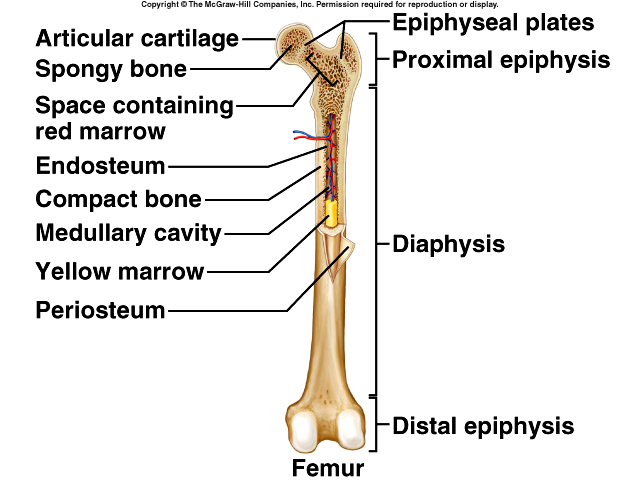
-
Diaphysis: shaft of a long bone
-
Epiphyses: the extremities at ends of the bone
-
Metaphysis: the region in the long bone where the diaphysis joins the epiphysis
-
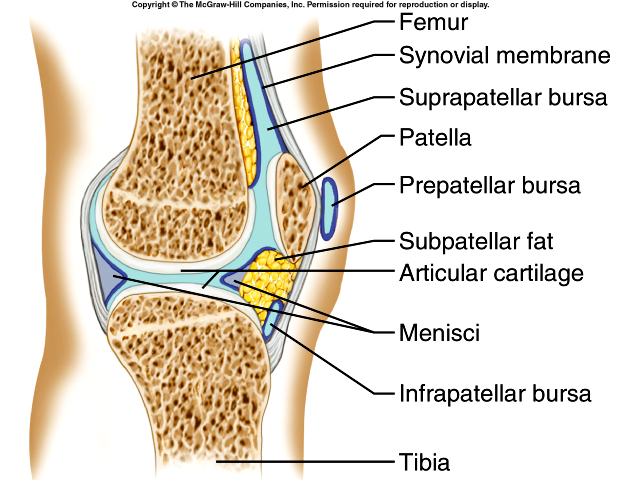
Articular Cartilage: thin layer of hyaline cartilage covering the epiphysis
-
Periosteum: membrane around the surface of the bone not covered by articular cartilage
-
Medullary or Marrow Cavity: space within the Diaphysis that contains yellow marrow
-
Endosteum: membrane that lines the Medullary cavity
HISTOLOGY OF BONE TISSUE
The cell types found in bone tissue are the osteogenic or osteoprogenitor cells (base cell
from which all connective tissue is derived), the osteoblasts (cells that form
bone, yet can’t undergo mitosis; secrete collagen, and other components that
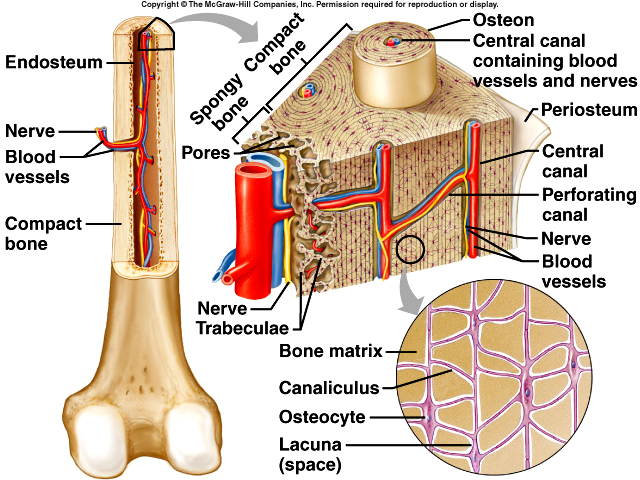
build bone), osteocytes (mature bone cells and principle cells of bone tissue
that reside in tiny cavities called lacunae),
and osteoclasts which function in bone resorption.
{kind=link}
Compact Bone tissue consists of osteons with little space between them. They lie over spongy bone and compose most of the bone tissue of the diaphysis. Its function is to support, protect and resists stress of weight.
Spongy Bone tissue on the other hand does not contain osteons, consists of trabeculae surrounding many red marrow filled spaces, and forms most of the structure of short, flat, and irregular bones, and the epiphysis of long bones. Its function is to store red marrow and provide some support.
Bone Marrow refers to the soft tissue that occupies the medullary cavity of long bones and the trabeculae of spongy bones and in the larger central canals. Red bone marrow is hemopoietic tissue and thus makes blood cells. Yellow bone marrow is red bone marrow that has turned fatty in young to middle-aged adults and serves as an energy storage.
PHYSIOLOGY OF BONE FORMATION: OSSIFICATION – Bone tissue is constantly rebuilding and changing shape. There are two types of ossification; intamembranous and endochondral. In intamembranous Ossification, bone formation is directly on or within the fibrous connective tissue membranes. This is easily seen in the skull bones and inside layer of the periosteum. It occurs within fibrous membranes of the embryo and the adult. At the site where bone will develop, mesenchymal cells become vascularized, cluster, and differentiate into osteoprogenitor cells and then into osteoblasts which secrete the organic matrix of bone. As the matrix forms, it develops trabeculae and the trabeculae from various centers fuse together to form spongy bone. On the outside of the bone, vascularized mesenchyme develops into the periosteum. Some of the spongy bone will be replaced by compact bone.
{kind=link}
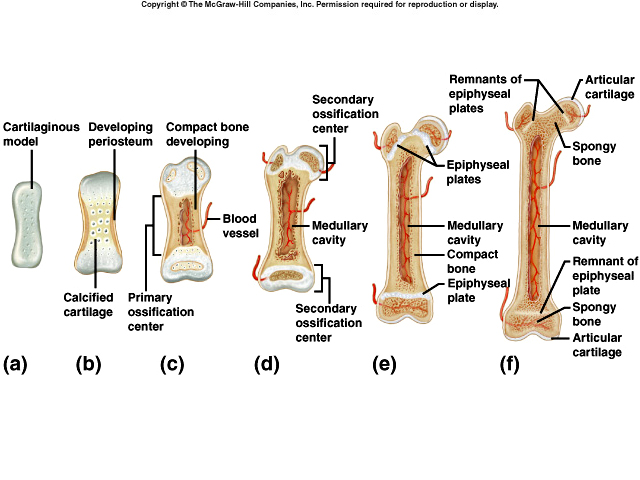
In endochondral ossification formation of bone occurs within a cartilage model. Most bones form this way. The primary ossification center of a long bone is in the diaphysis. Cartilage degenerates, leaving cavities that merge to form Medullary cavity. Osteoblasts lay down bone. Next, ossification occurs in the epiphysis, where bone replaces cartilage, except for the epiphyseal plate.
PHYSIOLOGY OF BONE
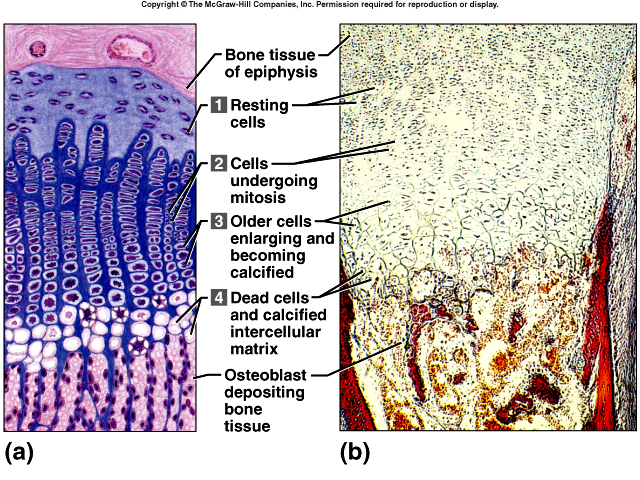
GROWTH AT THE EPIPHYSEAL PLATE
An epiphyseal plate consists of layers of cells: resting cells, young
dividing cells, older enlarging cells, and dying cells. The epiphyseal plate is
responsible for lengthening of the bone. Long bones tend to lengthen until the
epiphyseal plate ossifies. (Appositional growth) Growth in diameter is a
result of the addition of new bone tissue by periosteal osteoblasts around the
outer surface of the bone.
{kind=link}
BONE HOMEOSTASIS
Bone is living tissue that is constantly changing.
Bone Remodeling is the ongoing replacement of old bone tissue by new bone
tissue. Even after bone reaches adult shape and size, old bone is destroyed and
new bone is formed in its place. Old, worn and injured bone is removed and new
bone is laid down. Old bone is destroyed by osteoclasts and new bone is
constructed by osteoblasts. The body requires minerals, vitamins, and
hormones for this to happen. Foe example, the distal end of the femur is
replaced about every four months. Remodeling renews bone tissue before
deterioration sets in and it is also the way that bone heals.
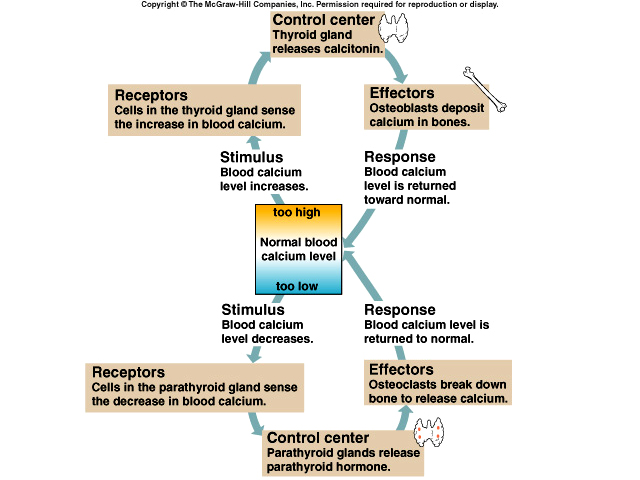
The Bone’s Role in
Calcium
Homeostasis
Bone is the major reservoir of Ca++. Bone “buffers” blood calcium levels by
releasing calcium when blood levels decrease and taking calcium back when blood
levels rise. Hormones that affect homeostasis of bone tissue are parathyroid
hormone which increases blood calcium levels by taking Ca++ from the bones and calcitonin which decreases blood calcium levels by depositing Ca++
back into the bones. Calcium is used in muscle and nrvous system physiology.
{kind=link}
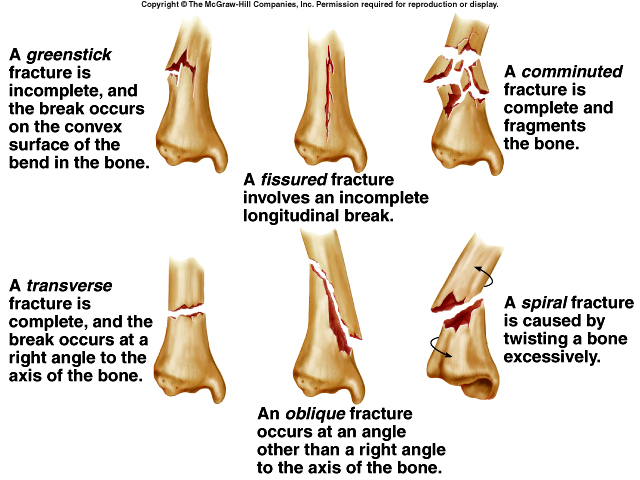
Fracture and
Bone Repair
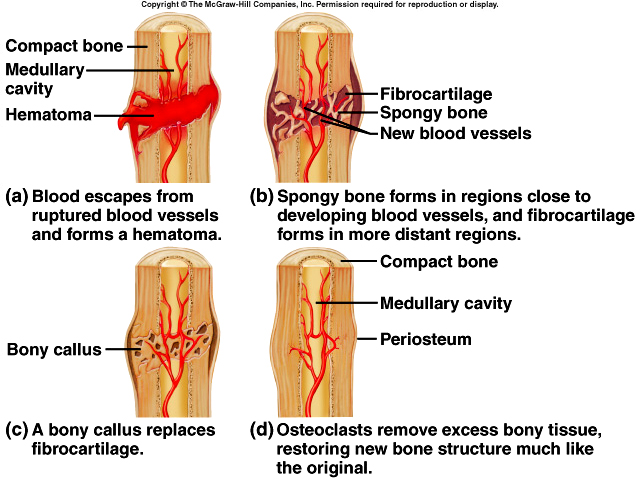
A fracture is any break in the bone. A closed reduction refers to setting a
bone to its original position by manipulation without surgery whereas an open
reduction refers to setting the bone during surgery. Repair involves formation
of a fracture hematoma, fibrocartilaginous callus (formation of granulation
tissue), bony callus and remodeling. A
fracture of the epiphyseal plate in a young person may delay or even halt bone
growth.
{kind=link}
{kind=link}
EXERCISE AND BONE
Bone can alter its strength in response to mechanical stress. Removal of stress
weakens bone through demineralization and collagen reduction.
AGING AND BONE TISSUE
The principle effect of aging is the loss of calcium in the bones which may result in
osteoporosis. A second effect is decreased production of matrix which makes
bones susceptible to fracture.
THE SKELETAL SYSTEM: THE AXIAL SKELETON
SURFACE MARKINGS
On the surface of bones there are many ridges, spines, bumps, canals, and holes.
Depressions receive other bones and openings allow blood vessels and nerves to
pass into bone. Processes form joints and serve as points of muscle attachment.
A list of all the surface features can be seen in table 8.2 of your text.
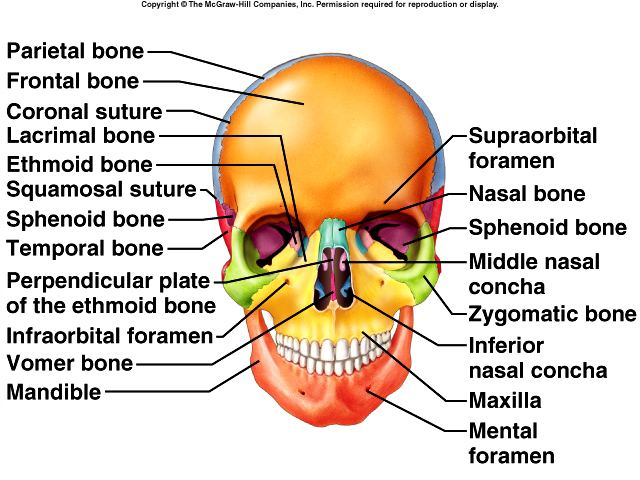
SKULL
The skull contains 22 bones (8 cranial and 14 facial). It rests on the
superior end of the vertebral column. The cranial bones enclose and protect
brain and include a frontal bone, parietal bones (2), temporal bones (2),
occipital bone, sphenoid bone, and ethmoid bone.
 The
frontal bone is
the forehead bone. It contains frontal sinuses that lie deep within. These
sinuses serve as sound chambers that give voice resonance. The parietal bones
form most of the sides and roof of the cranial cavity. The temporal bones form
the inferior sides of the cranium and part of the cranial floor. Within the
cranium the brain is housed in a space called the cranial fossa. The cranial fossa
can be divided into three sections (anterior, middle, posterior) accommodate
different compartments of the brain.
The
frontal bone is
the forehead bone. It contains frontal sinuses that lie deep within. These
sinuses serve as sound chambers that give voice resonance. The parietal bones
form most of the sides and roof of the cranial cavity. The temporal bones form
the inferior sides of the cranium and part of the cranial floor. Within the
cranium the brain is housed in a space called the cranial fossa. The cranial fossa
can be divided into three sections (anterior, middle, posterior) accommodate
different compartments of the brain.
{kind=link}
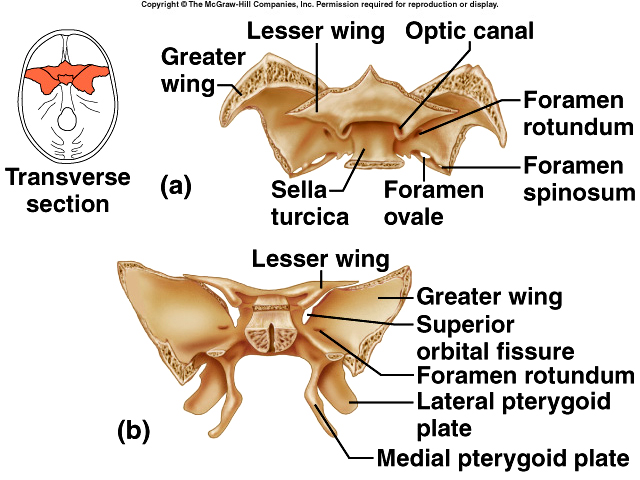
The Sphenoid bone lies at the middle part of the base of the skull articulating with all other cranial bones and holding them together. It forms part of the floor, side walls and rear wall of the orbits. It contains the sphenoid sinuses which drain into the nasal cavity. The greater/lesser wings, sella turcica, optic foramen, superior orbital fissure, pterygoid processes are all found on the sphenoid bone. Other structures and foramen on the sphenoid bone include the carotid foramen, jugular foramen, mastoid foramen, mandibular fossa, articular tubercle, internal and external auditory meatus, and the styloid process.
{kind=link}
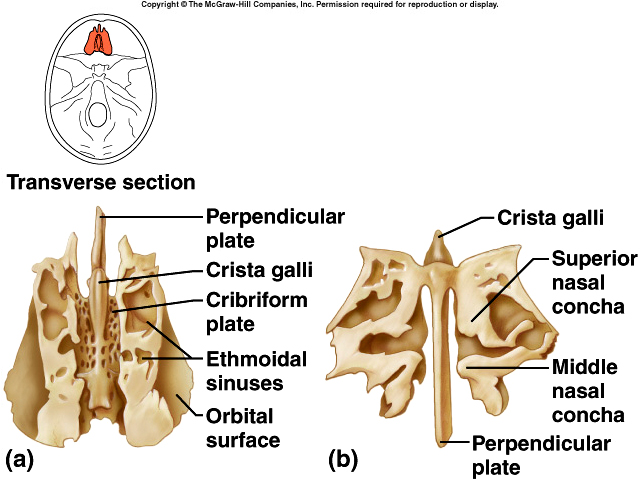
The Ethmoid Bone is a spongelike bone located between orbits. It forms part of the anterior portion of the cranial floor, the media wall of the orbits, superior portions of the nasal septum, most of the sidewalls of the nasal roof. Spaces in bone form ethmoid sinuses. Arising from the cribiform plate is the crista galli which serves as a point of attachment for the meninges that cover the brain.
{kind=link}
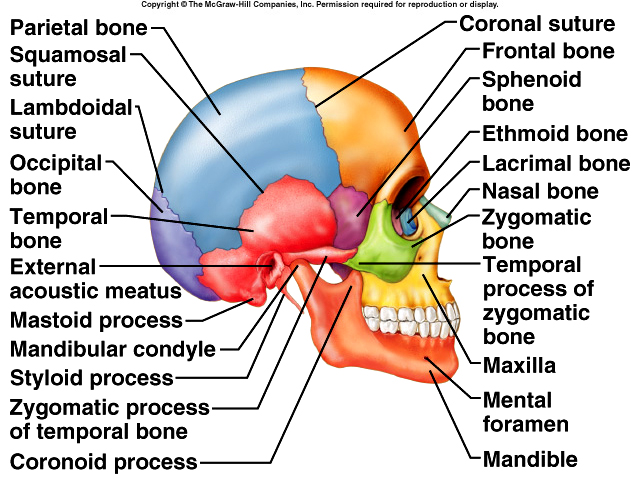
The petrous portion on the floor of the cranial cavity houses the middle and internal ear and the mastoid process serves as a point of attachment for several neck muscles. The occipital bone is the posterior part of the skull and most of the base of the cranium. It contains the foramen magnum through which the medulla oblongata passes. The occipital condyles, hypoglossal canal, external occipital protuberance are located on the occipital bone.
The facial bones have no direct contact with the brain or the meninges. The facial bones include nasal bones (2), maxillae (2), palatine bones (2), zygomatic bones (2), lacrimal bones (2), inferior nasal chonchae (2), vomer, and mandible. The nasal bones form the bridge of the nose. The maxillae unite to form the upper jawbone and it articulates with every bone in the face except the mandible. It contains maxillary sinuses. The roots of teeth reside in a deep socket called an aveolus. The Palatine bones form posterior portion of the hard palate. The zygomatic process joins with the zygomatic bone to form the zygomatic arch (cheekbones). The Lacrimal bones are the smallest bones in the face. The Vomer forms inferior and posterior part of the nasal septum. Inferior nasal chonchae (turbinates) allow more surface area in the nasal cavity.Paranasal sinuses are paired cavities found in the frontal, sphenoid, ethmoid and maxillae.
The Orbits of the eye are formed by seven bones of the skull: frontal, sphenoid, palatine, zygomatic, lacrimal, ethmoid, and maxilla.
The Mandible or lower jawbone contains a body, rami, condylar process (articulates with fossa of temporal bone), coronoid process (for muscle attachment), mandibular notch, and alveolar process. There are two foramen of note: the mental and mandibular. Foramina in all bones allow communication for blood, lymph, and neural information, between the interior and exterior of the skull.
Finally, the Hyoid Bone does not articulate with any other bone, but supports the tongue and provides attachment for muscles of the neck and pharynx.
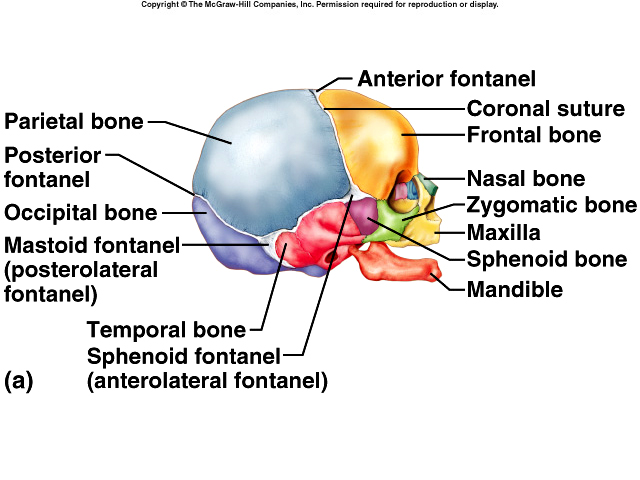
Fontanels are dense, connective tissue membrane-filled spaces between the cranial bones of fetuses and infants. These are also called the “soft spots” on an infants head. They enable the infant’s head to modify its size and shape as it passes through the birth canal and permits rapid growth of the brain during infancy. They also allow the physician to gauge the degree of brain development by their state of closure. The anterior (frontal) is located between the angles of two parietal bones and two segments of the frontal bone. The posterior occipital is found between two parietal bones and the occipital bone. Anterolateral (sphenoidal) are on each side of the skull at the juncture of the frontal, parietal, temporal, and sphenoid bones and posterolateral (mastoid) are located on each side of the skull at the junction of the parietal, occipital, and temporal bones.
{kind=link}
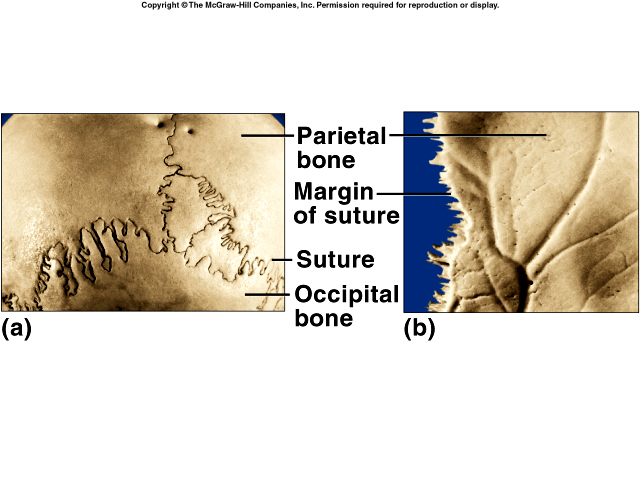
Sutures
A suture is an immovable joint. The cranial sutures include a coronal suture
which is between frontal bone and two parietal bones, a sagittal suture found
between two parietal bones, a lambdoid suture between parietal bone and
occipital bone, and a squamous suture between parietal bones and temporal bones.
{kind=link}
VERTEBRAL COLUMN
The vertebral column along with the sternum and the ribs form the skeleton
of the trunk of the body.
 Its function is to enclose and protect the spinal
cord, supports the head, and serves as a point of attachment for the ribs and
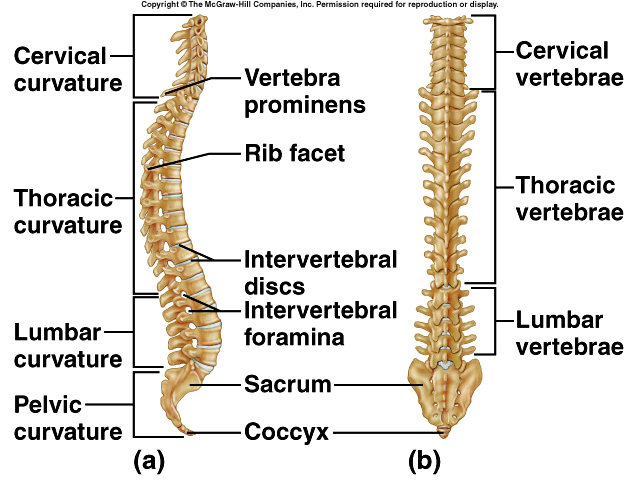
muscles of the back. The vertebral column is composed of seven
cervical
vertebrae, twelve thoracic vertebrae, five lumbar vertebrae,
five sacral vertebrae which fuse into one bone (sacrum), and four
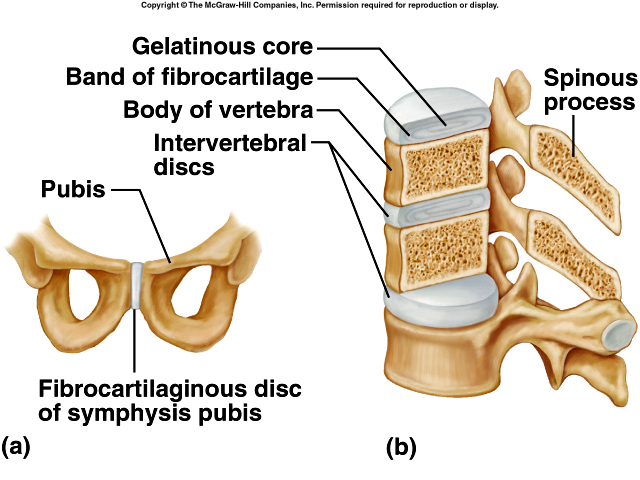
coccygeal vertebrae which fuse into two bones (coccyx). Between vertebrae are
intervertebral discs, the outer portion consists of fibrocartilage and is called
annulus fibrosus. A soft, elastic inner portion called nucleus pulposus. These
discs form strong joints, permits various movements and absorbs vertical shock.
Its function is to enclose and protect the spinal
cord, supports the head, and serves as a point of attachment for the ribs and
muscles of the back. The vertebral column is composed of seven
cervical
vertebrae, twelve thoracic vertebrae, five lumbar vertebrae,
five sacral vertebrae which fuse into one bone (sacrum), and four
coccygeal vertebrae which fuse into two bones (coccyx). Between vertebrae are
intervertebral discs, the outer portion consists of fibrocartilage and is called
annulus fibrosus. A soft, elastic inner portion called nucleus pulposus. These
discs form strong joints, permits various movements and absorbs vertical shock.
{kind=link}
{kind=link}
{kind=link}
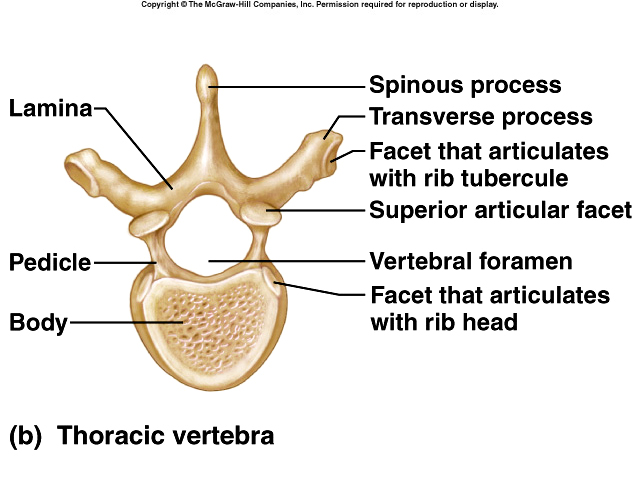
Normal Curves of the vertebral column increase strength, help maintain balance in the upright position, absorb shocks from walking, and protects the column from fracture. The primary (thoracic and sacra or pelvis) is anteriorly concave and the secondary (cervical and lumbar) is anteriorly convex. The cervical curve develops when baby holds his head up and the lumbar curve develops when baby stands.
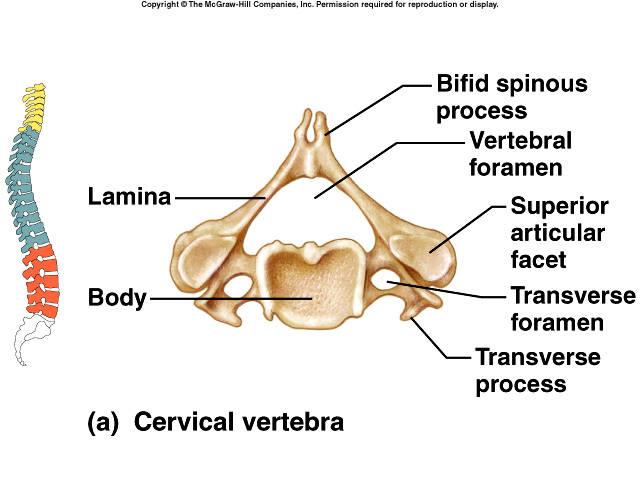
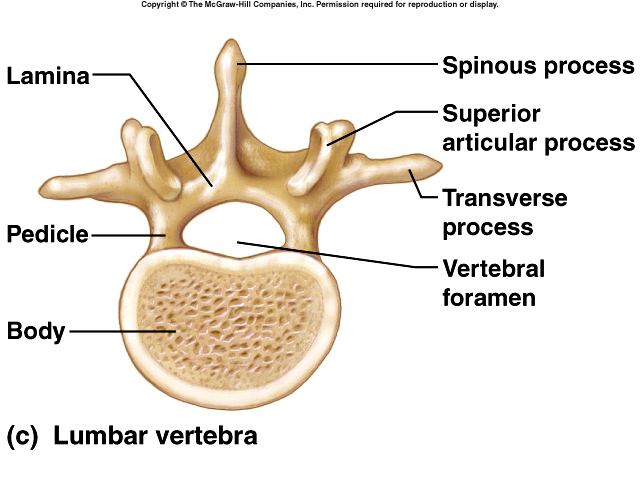
Typical Vertebrae have a body, the thick, disc-shaped portion that bears the weight, and a vertebral arch that extends posterior to the body and with the body surrounds the spinal cord. The arch is formed from the pedicles and laminae. Processes that arise from vertebral arch are the transverse and spinous and are used for muscle attachment. The superior articular (2) and the inferior articular (2) facets form joints with other vertebrae.
The first cervical vertebra (C1) is
the atlas. Its articulation permits head to signify yes. The second cervical
vertebra (C2), is called the axis, and it contains a structure (dens) that
permits to rotate, signifying no. In the Thoracic Region, the twelve bones are
larger and stronger than cervical vertebrae. Here the facets and demifacets
articulate with the ribs. The five bones of Lumbar Region are the largest and
strongest vertebrae because of their role in the support of the body’s weight.
The Sacrum, a triangular bone formed by fusion of 5 bones, serves as foundation
of pelvic girdle. The sacral promontory (superior border of sacrum) is used as
obstetrical landmark; the auricular surface articulates with ilium of each
hipbone. The Coccyx is the tailbone. The vertebral foramen houses the spinal
cord. The intervertebral foramen permits passage of a single spinal nerve
between the vertebrae. The transverse foramen allows vertebral artery, vein and
nerve to pass through as does the anterior and posterior sacral foramen.
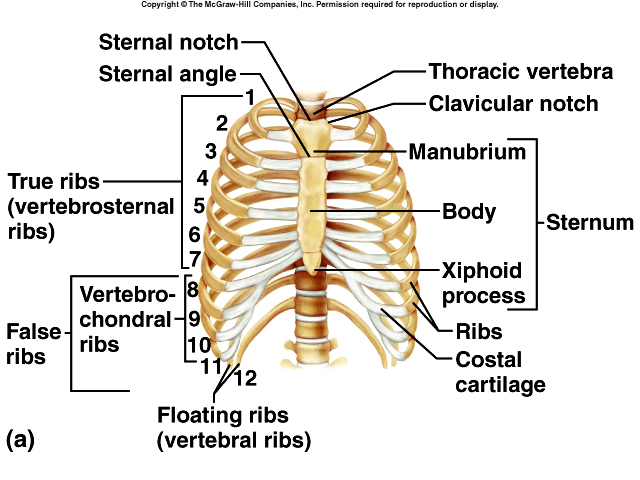
The function of skeleton of the THORAX is to enclose and protect organs in the
thoracic cavity and upper abdomen and to provide support for bones of the
shoulder girdle and upper extremities. It consists of the Sternum or breastbone.
Sections of the sternum are labeled manubrium, body, and xiphoid process. The
body of the sternum articulates with the second through tenth ribs. There are
twelve pairs of Ribs. The first through seventh (vertebrosternal ribs) pair
attach directly to sternum by a strip of hyaline cartilage (coastal cartilage)
and are the true ribs. Pairs 8-10 are called false ribs (vertebrochondral ribs)
because their coastal cartilage’s either attach indirectly to sternum or not at
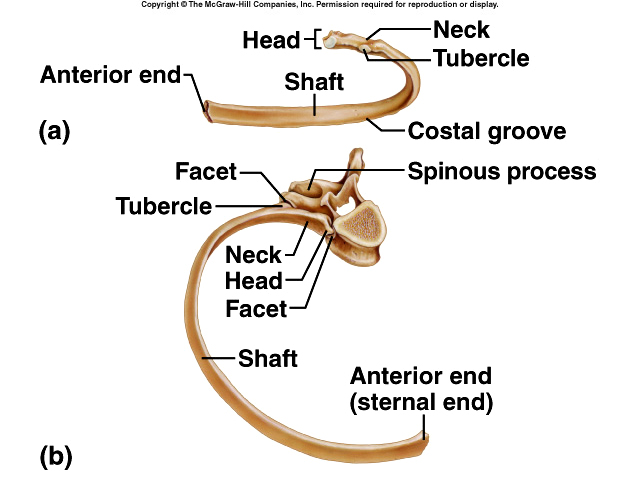
all (floating ribs, 11-12). The ribs may be labeled head, neck, coastal angle,
coastal groove.
{kind=link}
{kind=link}
THE APPENDICULAR SKELETON
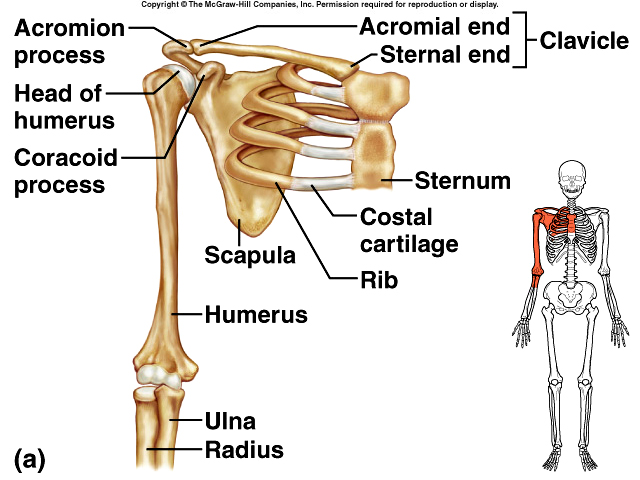
The PECTORAL (SHOULDERED) GIRDLE attaches the bones of the upper extremities to the axial skeleton and supports the shoulder. The Clavicle serves as a brace to keep the arm away from the thorax. It has two curves (one convex, one concave); juncture of these curves is where most fractures to the clavicle occur. The Scapula (shoulder blade) are broad triangular bones with spines, acromium processes (articulates with the clavicle), bodies, coracoid processes, glenoid cavities (fossa) receives the head of the humerus. They provide many points for muscle attachment.
{kind=link}
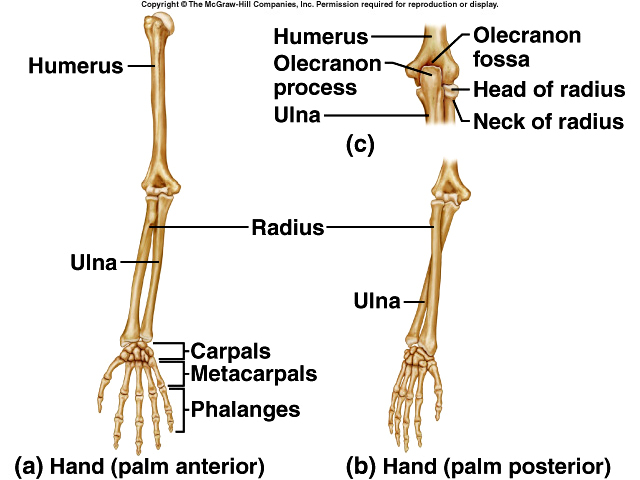 The UPPER EXTREMITY consists of 60
bones (thirty per limb) that provide the framework for muscle attachment and functions in levers
that move the limb and its parts. The Humerus is the longest bone in the upper
extremity. It has a head (proximal end), anatomical neck (former site of the
epiphyseal plate), greater and lesser tubercle and intertubercular sulcus,
deltoid tuberosity (point of attachment for deltoid muscle), a capitulum
(articulates with the head of the radius) radial fossa (receives the head of the
radius when forearm is bent), a trochlea: looks like a spool (articulates with
the ulna), and a coronoid fossa (receives part of the ulna when forearm is
bent), body (main shaft), olecranon fossa (receives olecranon when forearm is
extended), medial (“funny bone”) and lateral epicondyles (point of muscle
attachment). The surgical neck is the site of most fractures.
The UPPER EXTREMITY consists of 60
bones (thirty per limb) that provide the framework for muscle attachment and functions in levers
that move the limb and its parts. The Humerus is the longest bone in the upper
extremity. It has a head (proximal end), anatomical neck (former site of the
epiphyseal plate), greater and lesser tubercle and intertubercular sulcus,
deltoid tuberosity (point of attachment for deltoid muscle), a capitulum
(articulates with the head of the radius) radial fossa (receives the head of the
radius when forearm is bent), a trochlea: looks like a spool (articulates with
the ulna), and a coronoid fossa (receives part of the ulna when forearm is
bent), body (main shaft), olecranon fossa (receives olecranon when forearm is
extended), medial (“funny bone”) and lateral epicondyles (point of muscle
attachment). The surgical neck is the site of most fractures.
The Ulna and is longer than the Radius and overlaps the humerus posteriorly. It has a trochlear notch (receives the trochlear and separates the olecranon and coronoid processes), olecranon, and radial notch (receives the head of the radius).
The bones of the hand consist of Carpals, Metacarpals, and Phalanges. The Carpals are eight bones called scaffold, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate, and hamate. The five bones called metacarpals form the palm of the hand. Each bone has a proximal base, shaft, and distal head. The fourteen bones of the fingers are called the phalanges. Each has a base, shaft, and head. There are three per finger (phalanx), two bones in the thumb (pollex).
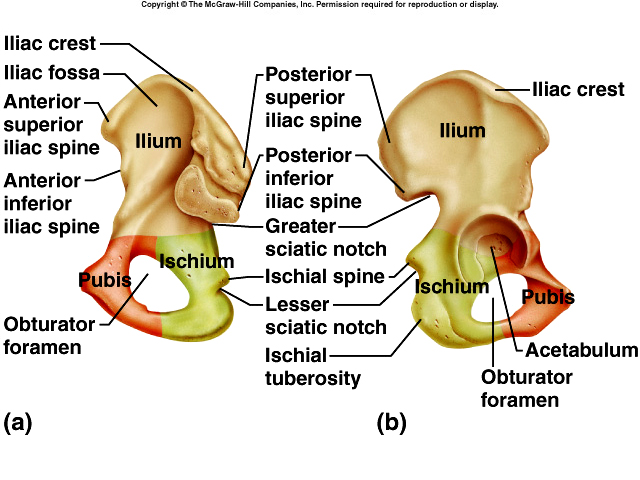
PELVIC (HIP) GIRDLE
The pelvic girdle consists of two hipbones or coxal bones
 joined anteriorly at
the pubic symphysis. At birth there are three separate bones (ilium, ischium and
pubis) but fuse to form one bone. The ilium is the superior bone, contains the
iliac crest, anterior and posterior superior and inferior iliac spine, greater
sciatic notch and iliac fossa. The auricular surface articulates with the sacrum
to form the sacroiliac joint. The ischium is the middle bone. Prominent features
include a ischial spine, lesser sciatic notch, ischial tuberosity, and a
obturator foramen (largest foramen in the skeleton). The ramus joins with the
pubis. The pubis is the anterior bone. It has a superior and inferior ramus,
body, and a pubic crest (anterior border) and pubic tubercle (on lateral end).
The acetabulum is a fossa formed by the ilium, ischium and pubis. It functions
as a socket for the head of the femur. Together the hipbones, sacrum and coccyx
form the pelvis. The pelvic brim is a plane marked by sacral promontory and the
arcuate lines of the ilia. It also is the superior most margin of the true
pelvis. The portion above pelvic brim is called the greater or (false) pelvis.
The portion below pelvic brim is known as the lesser (true) pelvis. It surrounds
the pelvic cavity. The superior opening of lesser pelvis is called the pelvic
inlet and is the pelvic brim whereas the inferior opening is the pelvic outlet.
In females the outlet is wide and oval shaped and in males it is narrower and
heart shaped. The pelvis axis is the course taken by baby’s head as it descends
through the pelvis.
joined anteriorly at
the pubic symphysis. At birth there are three separate bones (ilium, ischium and
pubis) but fuse to form one bone. The ilium is the superior bone, contains the
iliac crest, anterior and posterior superior and inferior iliac spine, greater
sciatic notch and iliac fossa. The auricular surface articulates with the sacrum
to form the sacroiliac joint. The ischium is the middle bone. Prominent features
include a ischial spine, lesser sciatic notch, ischial tuberosity, and a
obturator foramen (largest foramen in the skeleton). The ramus joins with the
pubis. The pubis is the anterior bone. It has a superior and inferior ramus,
body, and a pubic crest (anterior border) and pubic tubercle (on lateral end).
The acetabulum is a fossa formed by the ilium, ischium and pubis. It functions
as a socket for the head of the femur. Together the hipbones, sacrum and coccyx
form the pelvis. The pelvic brim is a plane marked by sacral promontory and the
arcuate lines of the ilia. It also is the superior most margin of the true
pelvis. The portion above pelvic brim is called the greater or (false) pelvis.
The portion below pelvic brim is known as the lesser (true) pelvis. It surrounds
the pelvic cavity. The superior opening of lesser pelvis is called the pelvic
inlet and is the pelvic brim whereas the inferior opening is the pelvic outlet.
In females the outlet is wide and oval shaped and in males it is narrower and
heart shaped. The pelvis axis is the course taken by baby’s head as it descends
through the pelvis.
The LOWER EXTREMITY consists of sixty bones (again, thirty
per limb).
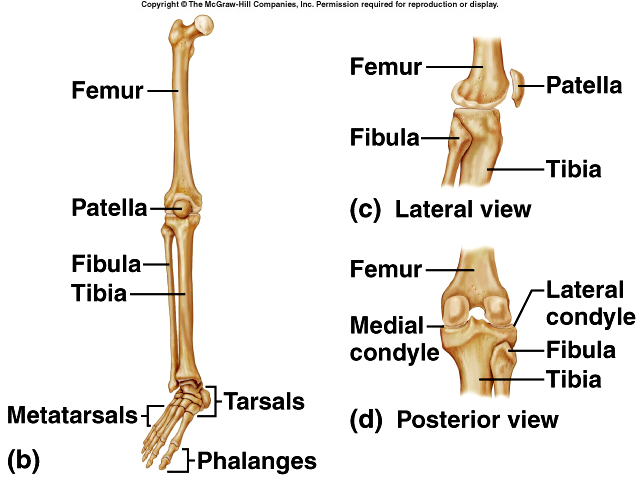 The Femur or thighbone is longest, heaviest, and strongest bone in the body. The
proximal portion (head) articulates with the hip bone, distal end articulates
with the tibia. The body is the shaft. It has a linea aspera (ridge that serves
as attachment point for thigh muscles), a neck (most of the fractures in elderly
patients occur here), greater and lesser trochanter (serve as points of
attachment for muscles), distal end has medial and lateral condyles which
articulate with tibia, medial and lateral epicondyles which lie above condyles,
and a fovea capitis (a depression in the head of the femur to which is attached
a ligament that joins to the acetabulum). The Patella is the kneecap.
The Femur or thighbone is longest, heaviest, and strongest bone in the body. The
proximal portion (head) articulates with the hip bone, distal end articulates
with the tibia. The body is the shaft. It has a linea aspera (ridge that serves
as attachment point for thigh muscles), a neck (most of the fractures in elderly
patients occur here), greater and lesser trochanter (serve as points of
attachment for muscles), distal end has medial and lateral condyles which
articulate with tibia, medial and lateral epicondyles which lie above condyles,
and a fovea capitis (a depression in the head of the femur to which is attached
a ligament that joins to the acetabulum). The Patella is the kneecap.
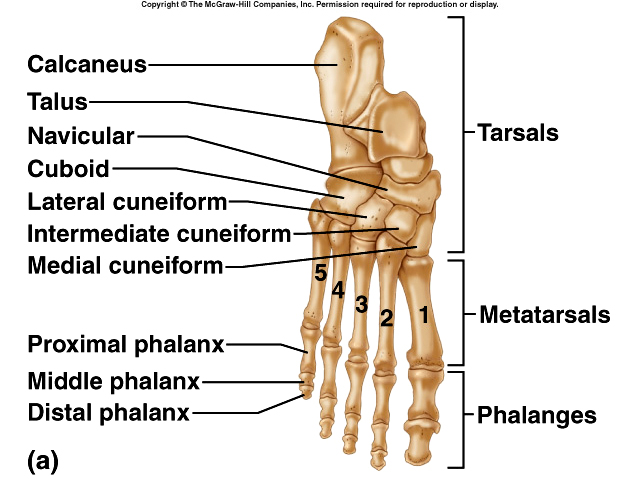
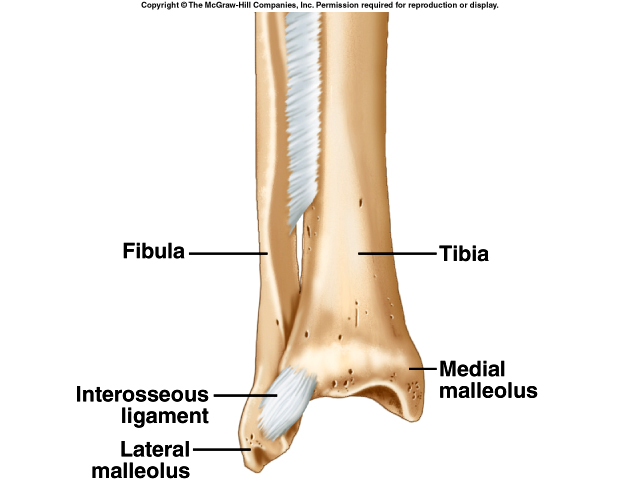
The Tibia (shinbone) bears most of the weight of the leg. It has lateral and medial condyle at proximal end articulate with the femur. The tibial tuberosity is a point of attachment for the patellar ligament. It medial malleolus can be located as the inner bulge of ankle and the fibular notch articulates with end of fibula. The fibula is parallel and lateral to the tibia. It does not articulate with the knee and the lateral malleolus is outside bilge of ankle.
The Tarsus, Metatarsals, and Phalanges make up the bones of the ankle and foot. The bones of the ankle are the talus (only bone that articulates with the fibula and tibia), calcaneus, cuboid, navicular, three cuneiforms and the calcaneus (heel bone which is largest and strongest tarsal bone). The metatarsals consist of five bones. The phalanges of the foot, like the metatarsals, have a base, shaft and head. The hallux is the great toe. There is a longitudinal arch and transverse arch provide support and leverage to foot.
{kind=link}
FEMALE AND MALE SKELETONS
Male bones are usually larger and heavier than female bones and have more
prominent makings for muscle attachment. The female pelvis is adapted for
pregnancy and childbirth and is wider, shallower, lighter, and rounder than the
male pelvis.
DISORDERS OF THE SKELETAL SYSTEM
Genetic disorders include Achondroplasia (an autosomal dominant trait which is
the most common inherited form of dwarfism), Osteopetrosis (nine rare inherited
disorders causing abnormally dense bone), osteogenesis imperfecta (a connective
tissue disease that affects the skeleton, child appears with many broken bones
suggesting child abuse).
Developmental or metabolic disorders include Scoliosis and kyphosis (curvature of the spine usually seen in adolescent girls), osteochondroma (developmental defect where bone grows away from the joint), osteoporosis (metabolic loss of bone tissue usually seen in older females) and Osteomalacia or Rickets (inadequate mineralization due to decreased Vitamin D). Osteomylitis is an infection in the bone. Tumors can be malignant (Osteosarcoma) or benign (Fibroma and osteoid osteoma). Metastatic tumors are those that originate in breast, prostate, lung, thyroid and kidney cancers and spread to the bone.
JOINTS OF THE SKELETAL SYSTEM
CLASSIFICATION OF JOINTS
(Articulations between Bones)
In Fibrous joints there is no joint cavity and the bones are held together by
fibrous connective tissue, (Immovable joints).
-
Syndesmosis: a fibrous joint that has more fibrous connective tissue (example is joint between distal articulation of tibia and fibula).
-
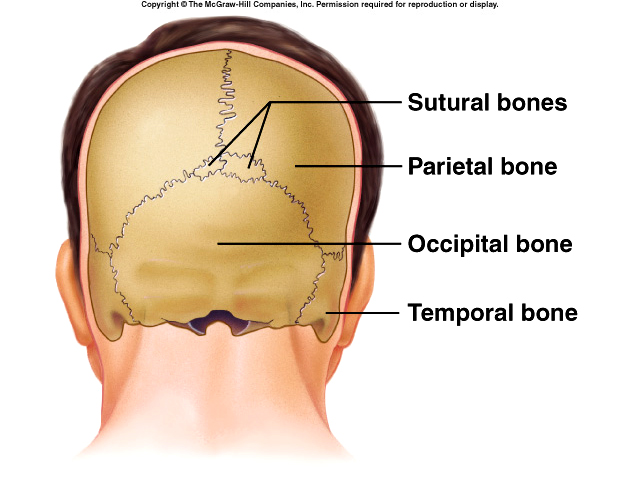
Sutures: a fibrous joint, thin layer of dense fibrous connective tissue that unites the bones of the skull; becomes a synostosis in adult (by complete fusion of bones across joint.
-
Gomphosis: a cone shaped peg fits into a socket (roots of teeth).
{kind=link}
{kind=link}
Bones held together by cartilage in Cartilaginous joints. These are slightly movable joint.
-
Synchondrosis: a cartilaginous joint in which the connecting joint is hyaline cartilage, this is only a temporary joint
-
Symphysis: a broad flat disc of fibrocartilage (outer area of intervertebral discs and pubic symphysis
{kind=link}
 In a Synovial joint, a synovial
cavity is present. Bones forming joint are united by a surrounding articular
capsule and frequently ligaments. Synovial joints are also known as Diarthrosis
or freely movable joints. Many diarthroses also contain articular discs
(menisci) and bursae. The factors that affect movement of diarthroses include
its structure or shape of the articulating bones, which determines how they fit
together, the strength and tension of the joint ligaments, the arrangement and
tension of the muscles, the apposition of the soft parts may limit mobility
(bent elbow) and the presence of hormones (relaxin).
In a Synovial joint, a synovial
cavity is present. Bones forming joint are united by a surrounding articular
capsule and frequently ligaments. Synovial joints are also known as Diarthrosis
or freely movable joints. Many diarthroses also contain articular discs
(menisci) and bursae. The factors that affect movement of diarthroses include
its structure or shape of the articulating bones, which determines how they fit
together, the strength and tension of the joint ligaments, the arrangement and
tension of the muscles, the apposition of the soft parts may limit mobility
(bent elbow) and the presence of hormones (relaxin).
Types of Synovial Joints
-
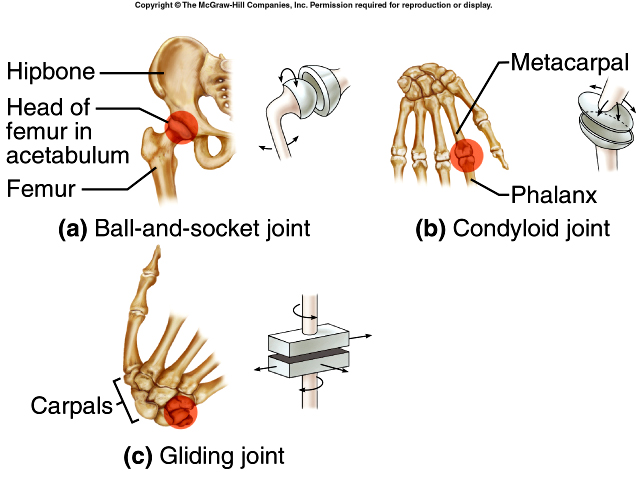
Ball-and-socket: ball-like surface of one bone fits into cuplike depression of another bone, triaxial movement (hip and shoulder).
-
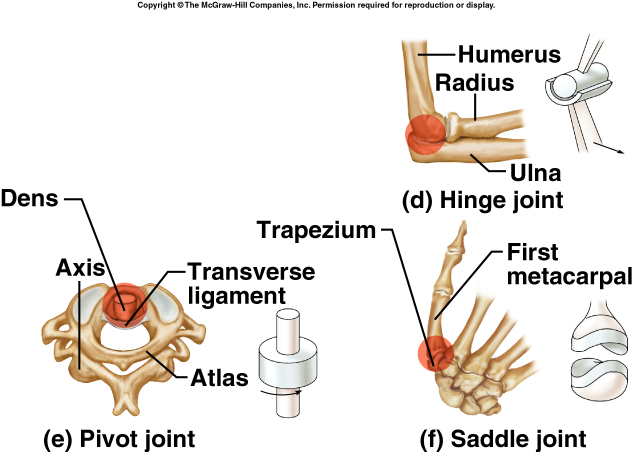
Hinge: convex surface of one bone fits into the concave surface of another bone, monaxial movement (elbow and phalanges).
-
Saddle: one bone is saddle shaped and other bone is shaped like legs of rider, metacarpal of thumb and carpel bone.
-
Pivot: a rounded or pointed surface of one bone articulates within a ring of another, movement is rotation, (atlas-axis, proximal ends of radius and ulna).
-
Gliding: side-to-side and back-and-forth movements (wrists and ankles).
-
Condyloid: oval shaped condyle of one bone fits into an elliptical cavity of another, biaxial movement, side-to-side and back-and-forth (between radius and carpals).
{kind=link}
{kind=link}
Common movements of joints
-
flexion: decrease in angle
-
extension: increase in angle
-
hyperextension: continuation of extension
-
abduction: movement of a bone away from midline
-
adduction: movement of a bone toward midline
-
circumduction: combination of flexion-extension & abduction-adduction special movements at diarthroses.
Special movements of joints
-
rotation: moving a part around an axis
-
elevation- depression: movement of part of the body upward/downward
-
protraction-retraction: movement of mandible forward or backward
-
inversion-eversion: movement of the sole of the foot inward/outward dorsiflexion-plantar flexion: bending of the foot upward/downward
-
supination-pronation: turns the palm of the hand anteriorly/superiorly or posteriorly/inferiorly
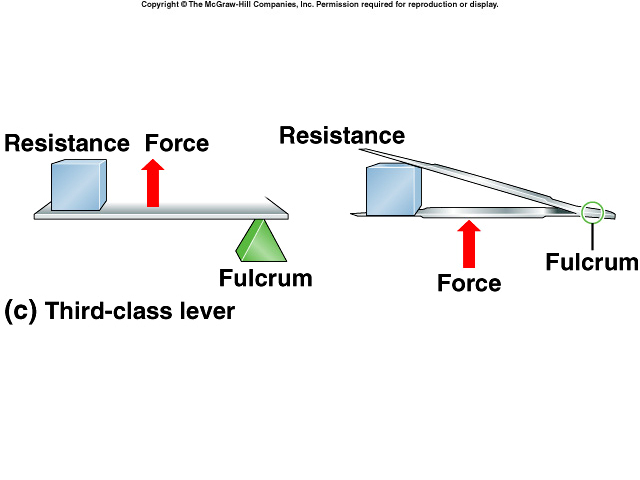
LEVERS AND BIOMECHANICS OF JOINTS
The functions of bone are to provide support and the framework for the body.
They serve as a point of attachment for muscles and protect the internal organs.
They help in movement because muscles are attached to the bones. Bones serve as
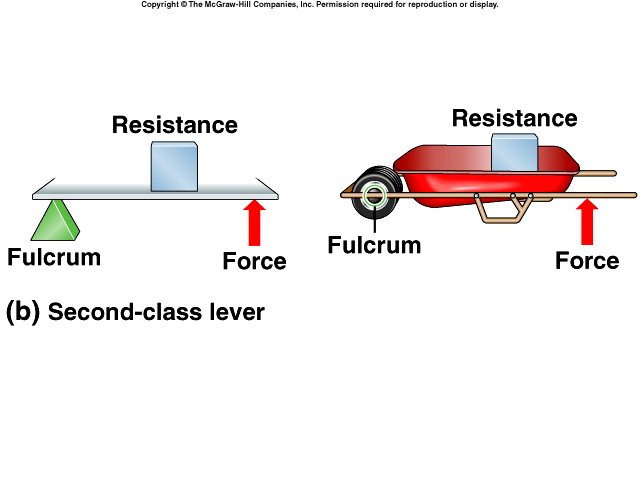
levers and joints serve as fulcrums (pivots). The lever is acted on by two
different forces: resistance and force or effort. Resistance is the force or weight that
opposes movement and effort is the force used to achieve an action. Leverage,
the mechanical advantage gained by a lever, is largely responsible for a muscles
strength and range of motion. In a first
class lever (RFE), fulcrum is between resistance and effort. There is only one
first class lever in the body. In the
second class
lever (FRE) resistance is between fulcrum and effort (levers of strength).
There is only one second class lever in the body. In
the third class lever (FER) effort is between fulcrum and resistance. This is
the most common lever in the body.
{kind=link}
{kind=link}
Special Joints
The shoulder joint (humeroscapular joint) is formed by head of humerus and the glenoid cavity of
scapula. It exhibits the most freedom of movement of all joints of the body.
Most of the strength results from muscles surrounding joint (rotator cuff).
The elbow joint (humeroulnar joint) contains a hinge joint and a gliding joint.
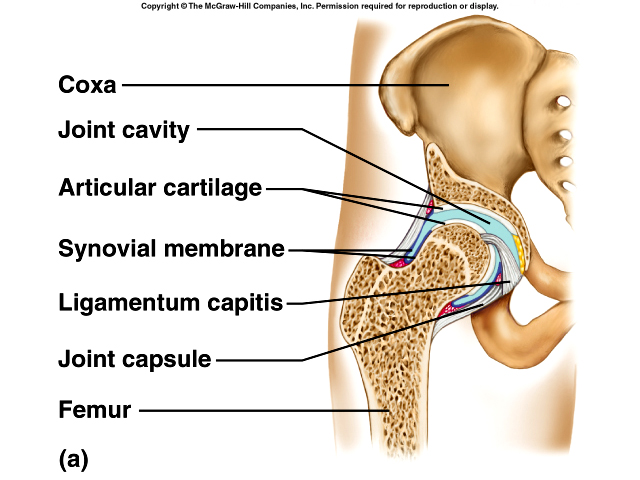
The hip joint (coxal joint) is formed by head of femur and acetabulum. The fovea capitis is a pit in head of femur where a ligament attaches the femur and the coxal bone together.
{kind=link}
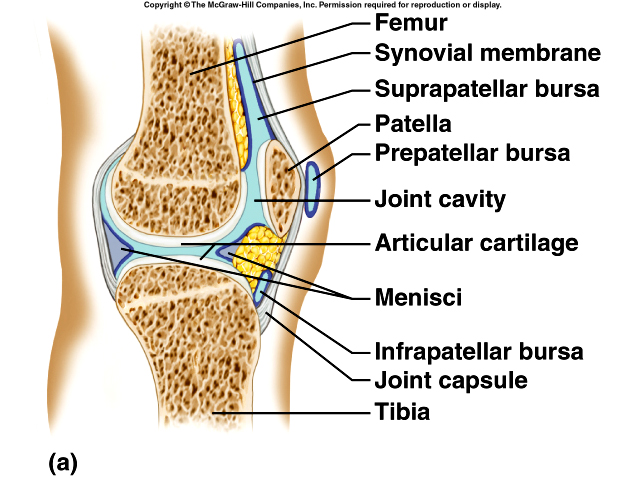
The knee joint is the most complex joint in the body and
the largest joint of the body. It consists of two condyloid joints and a gliding
joint. The presence of menisci compensate for the irregular shapes of the
articulating bones. Bursae are sacks of synovial fluid located at friction
points.
JOINT DISORDERS
A Dislocation is a displacement of a bone from a joint with tearing of
ligaments, tendons and articular cartilage. A sprain is the forcible wrenching
or twisting of a joint with partial rupture or other injury to its ligaments
without dislocation whereas a strain is the overstretching of the muscle around
a joint. Torn Cartilage. Bursitis can be either acute or chronic inflammation of
the bursa.
{kind=link}
Arthritis is inflammation of one or more joints. Rheumatoid arthritis is an autoimmune disease where the synovial membrane becomes inflamed and thickened, fibrous tissue infiltrates further restricting movement, and in time joints may ossify. Osteoarthritis is the most common type of arthritis that usually occurs with aging. The articular cartilage softens and disintegrates, roughing the articular surfaces. Lyme arthritis is caused by a bacteria Borrelia burgdorferi, which is transmitted by the deer tick. In Gout arthritis, uric acid crystals are deposited in the joints.
MUSCLE TISSUE
FUNCTIONS OF MUSCLE TISSUE
Motion, movement of substances within the body, stabilizing Body Positions
and Regulating Organ Volumes and Generation of Heat are the functions of the
muscular system.
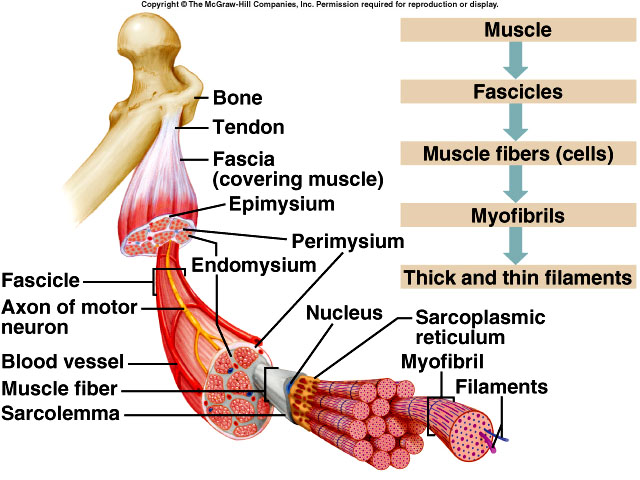
Connective
Tissue Components
Single muscle fibers are encased in a thin layer of connective tissue called
endomysium. Muscle fibers are grouped in bundles called fascicles which are
separated from other fascicles by another layer of connective tissue called
perimysium. The muscle as a whole is surrounded still by another layer of
connective tissue called epimysium which becomes fasciae - deep fasciae between
adjacent muscles and superficial fascia between the skin and muscles. All three
layers of connective tissue may extend beyond the muscle fiber as tendons (a
cord of dense connective tissue that attaches the muscle to the periosteum of a bone.
{kind=link}
SKELETAL MUSCLES
ACTIONS
Origin and Insertion
Skeletal muscles produce movement by exerting force on tendons, which in
turn pull on bones or other structures. Most muscles cross at least one joint
and are attached to the articulating bones of that joint. When a muscle
contracts it draws one articulating bone towards the other. The attachment to
the stationary bone is the origin. The attachment to the moveable bone is the
insertion.
Group Actions
Most movements are coordinated by several skeletal muscles acting in groups
rather than by themselves. Most skeletal muscles are arranged in opposing
(antagonistic) pairs at joints. A muscle that causes the desired action is the
agonist or prime mover; the antagonist produces the opposing action. Most
movements also involve muscles called synergists, which serve to steady a
movement, thus preventing unwanted movements and helping the prime mover
function more efficiently. Some synergist muscles in a group also act as
fixators, which stabilize the origin of the prime mover so that it can act more
efficiently. Under different conditions and depending on the movement and which
point is fixed, many muscles act, at various times, as prime movers,
antagonists, synergists, or fixators.
NAMING SKELETAL MUSCLES
Learning terms to indicate specific muscle characteristics will help one
remember muscle names. If one considers direction terms like transverse
(perpendicular to the midline), rectus (parallel to the midline) and oblique
(diagonally to the midline). If a prominent structure is near to where the
muscle is that location may be used in the muscle name. Size of the muscle, such
as maximus (large), minimus (small), longus (longest), and brevis (shortest) are
used. The number of origins the muscle has, i.e. biceps (2), triceps (3),
quadriceps (4) can be used to name muscles. A muscle may be named because of its
shape: deltoid (triangular), trapezius (trapezoid shape), serratus (saw-toothed
shape), and rhomboideus (diamond shape). A muscle may be named for where they
insert. Or the name may include the action they perform. See table 10.1 in your
text for more information on naming muscles.
- flexor (decrease angle at joint),
- extensor (increase angle at joint),
- abductor (moves a bone away from the midline),
- adductor (moves a bone toward the midline),
- levator (produces an upward movement),
- depressor (produces a downward movement),
- supinator (turns the palm upward),
- pronator (turns the palm downward),
- sphincter (decreases the size of an opening),
- tensor (makes a body part more rigid),
- rotator (moves a bone around its longitudinal axis).
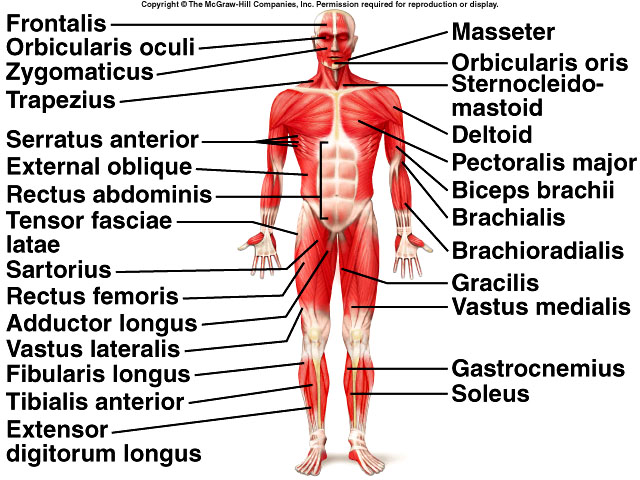
PRINCIPLE SKELETAL MUSCLES
The Muscles of Facial Expression provide the ability to express a variety of
facial emotions. The muscles lie within the superficial fascia and usually
originate in fascia or facial bones and insert into the skin and thus move the
skin rather than joints.
Muscles
-
Frontalis: draws scalp anteriorly, elevates eyebrows, wrinkles skin of forehead horizontally
-
Occipitalis: draws scalp posteriorly
-
Frontalis and occipitalis are part of epicranius muscle and are united by galea aponeurotica
-
Orbicularis oris: closes lips, compresses lips against teeth, protrudes lips and shapes lips during speech
-
Zygomaticus major: used in smiling or laughing
-
Buccinator: major cheek muscle used in blowing and sucking
-
Platysma: depresses mandible and also used in pouting
-
Risorius: draws angle of mouth laterally
-
Orbicularis occuli: closes eye
Muscles that Move the Lower Jaw are involved in chewing and biting. The muscles are the masseter, temporalis, medial and lateral pterygoid.
Muscles that Move the Eyeballs are extrinsic muscles originate outside the eyeball and move eyeball in various directions. Intrinsic muscles originate within the eye and move structures inside the eye.
Muscles that Move the Tongue
Extrinsic muscles originate outside the tongue and insert into it move the
tongue in various directions. Intrinsic muscles: originate within the tongue and
alters its shape.
Muscles that Move the Head include the sternocleidomastoid (draws head forward when both used or to one side or the other when only one is contracted), splenius capitis, semispinalis capitis and erector spinae.
Muscles that Move the Pectoral Girdle are the pectoralis minor, serratus anterior, trapezius, levator scapulae, rhomboideus major.
Muscles Used in Breathing are the diaphragm, external and internal intercostals.
Muscles that move the Humerus:
-
Flexors: coracobrachialis and pectoralis major
-
Extensors: teres major and latissimus dorsi
-
Abductors: suprapinatus and deltoid
-
Rotators: subscapularis, infraspinatus, and teres minor
Muscles that Move the forearm:
-
Flexors: biceps brachii, brachialis, brachioradialis
-
Extensors: triceps brachii
-
Rotators: pronator teres, and quadratus, supinator muscle

Muscles that Move the Wrist, hand and Fingers
-
Flexors: flexor carpi radialis, palmaris longus, flexor carpi ulnaris, flexor digitorum profundus and flexor digitorum superficialis
-
Extensors: extensor carpi radialis longus, extensor carpi radialis brevis, extensor digitorum, extensor carpi ulnaris
Muscles that Act on the Abdominal Wall
-
Rectus abdominis: flexes vertebral column and compresses abdomen
-
External and Internal oblique: compresses abdomen, enables lateral rotation
-
Transverse abdominis: compresses abdomen
Muscles of the Pelvic Floor include the levator ani, coccygeus, superficial transverse perini, bulbospongiousus, ischiocavernosus, and sphincter urethrae
Muscles that Move the Thigh
-
Anterior group: Psoas major, iliacus
-
Posterior group: gluteus (maximus, medius, minimus), tensor fasciae latae
-
Attach to femur: adductor magnus, pectineus, adductor longus, and gracilis
Muscles that move the leg:
-
Flexors: biceps femoris, semitendinosus, semimembranosus, satorius
-
Extensors: quadriceps femoris (rectus femoris, vastus lateralis, vastus medialis, vastus intermedius)
Muscles that Move the Foot and Toes
-
Dorsal flexors: tibialis anterior, extensor digitorum longus
-
Plantar flexors: tibialis posterior, gastrocnemius, soleus, flexor digitorum longus
-
Invertor: tibialis posterior
-
Evertor: Fibularis longus
CHARACTERISTICS OF MUSCLE TISSUE
Muscle tissue exhibits Excitability or the ability to respond to
certain stimuli by producing electrical signals called action potentials. The
ability of a muscle to propagate or conduct action potentials along the plasma
membrane is called Conductivity. Contractility is the ability to
shorten and thicken (contract), generate force to do work. Extensibility
is the ability to be extended (stretched) without damage to tissue. Finally,
Elasticity is the ability to return to original shape after contraction or
extension.
ANATOMY AND INNERVENTION OF SKELETAL MUSCLE TISSUE
Microscopic Anatomy of Skeletal
Muscle
Muscles are composed of many muscle fibers or myofibers. The plasma membrane
that separates fibers is called the sarcolemma. The fiber’s cytoplasm is called
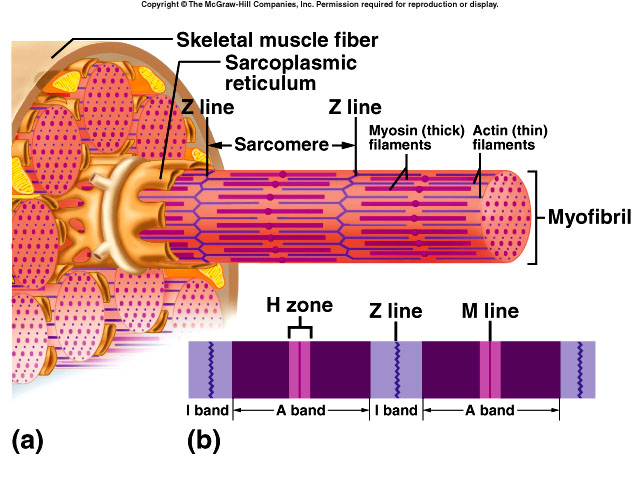
the sarcoplasm. The sarcoplasm contains much glycogen as stored energy. At high magnification the sarcoplasm
appears to be stuffed with little threads; these are the myofibrils. Myofibrils are the contractile
elements of skeletal muscle and contain three types of structures called
filaments or myofilaments (thin, thick, and elastic filaments). These filaments
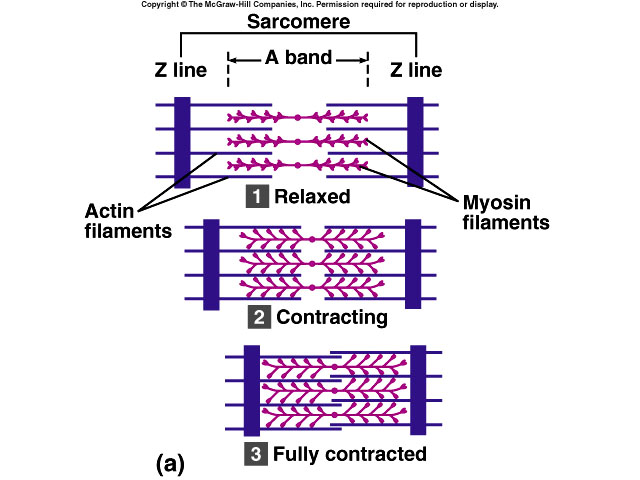
are arranged in compartments called sarcomeres.
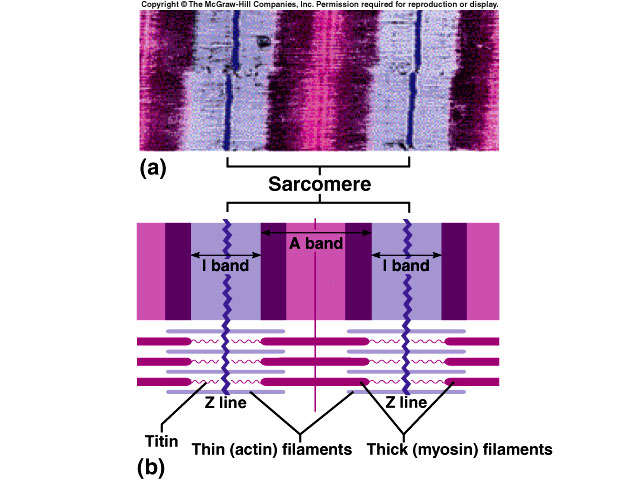
Z disc (lines) separate one sarcomere from another. A bands are the darker area composed of mostly of thick
filaments. I bands consist only of thin filaments and are lighter. H zones contain only thick
filaments and is at the center of the A band. The
contractile proteins are myosin which makes the thick filaments. The thin
filaments are composed of Actin, troponin and tropomyosin. Elastic filaments
contain titin which anchors the thick filaments to the Z disc. For more
information concerning the terminology of the components of a muscle fiber refer
to table 11.1 of your text.
{kind=link}
{kind=link}
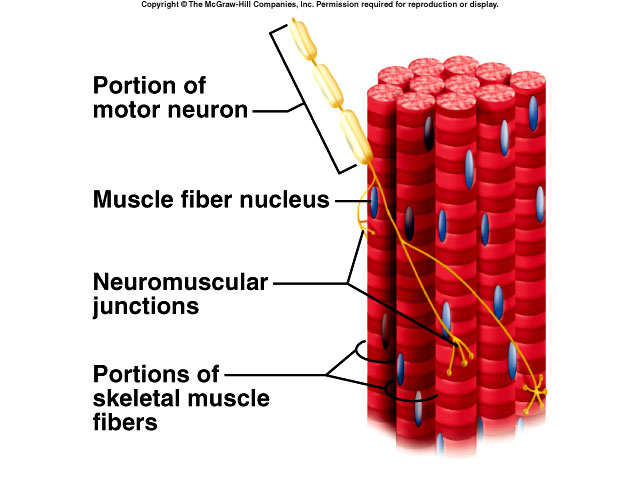
Nerves containing motor neurons convey impulses for muscular contraction. A motor neuron and the muscle fibers it stimulates form a motor unit. A single motor unit may innervate as few as ten or as many as 2,000 muscle fibers, with an average of 150 fibers being innervated by each motor neuron. The Neuromuscular Junction is the junction between a motor neuron and a muscle fiber. Excitable cells communicate with one another and other target cells at specialized regions called synapses. In most synapses there is a gap called a synaptic cleft. The first cell releases a neurotransmitter, acetylcholine, a chemical that bridges the gap. The neuromuscular junction will be covered in more detail in the next unit.
{kind=link}
CONTRACTION OF MUSCLE
Muscle contraction can be explained by the Sliding Filament Theory. In this
theory myosin heads pull on the thin filaments causing them to slide toward the
H zone. Sliding of the filaments causes a shortening of the muscle fibers and
the muscle. Calcium plays important role in muscular contraction, an increase in
the level of calcium in the sarcoplasm starts the movement of thin filaments.
ATP is required as the source of energy. Skeletal Muscles produce heat during
contraction. A portion of the heat released during muscular contractions helps
maintain normal body temperature. Excess heat is removed through the skin and
lungs.
MUSCLE RESPONSES
In the All-or-None Effect, a single action potential elicits a single
contraction in all the muscle fibers. Individual muscle fibers contract to their
fullest. Amount of tension (force) develops depends on the frequency of
stimulation of the muscle fibers by the neurons, the length of the muscle fiber
just before they contract, the number of muscle fibers contracting, and the
structural components of the muscle itself.
{kind=link}
{kind=link}
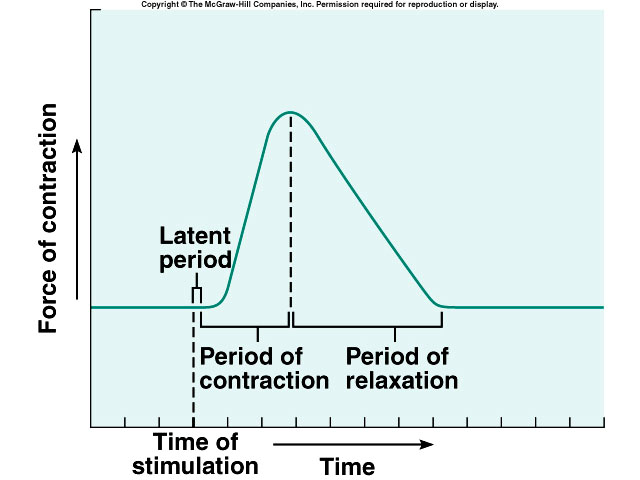
A Twitch Contraction is a
brief contraction of all the muscle fibers in a
 motor unit of a muscle in
response to a single action potential. During the Latent period Calcium is being
released. The latent period is followed by a Contraction period, then a
Relaxation period, and finally a Refractory period. The Refractory period can be
describes as follows. If two stimuli are applied one immediately after the
first, the muscle will respond only to the first, but not the second and will
not respond until the responsiveness of the muscle is retained. Usually this
time is about 5 milliseconds for skeletal muscle and 300 milliseconds for
cardiac muscle.
motor unit of a muscle in
response to a single action potential. During the Latent period Calcium is being
released. The latent period is followed by a Contraction period, then a
Relaxation period, and finally a Refractory period. The Refractory period can be
describes as follows. If two stimuli are applied one immediately after the
first, the muscle will respond only to the first, but not the second and will
not respond until the responsiveness of the muscle is retained. Usually this
time is about 5 milliseconds for skeletal muscle and 300 milliseconds for
cardiac muscle.
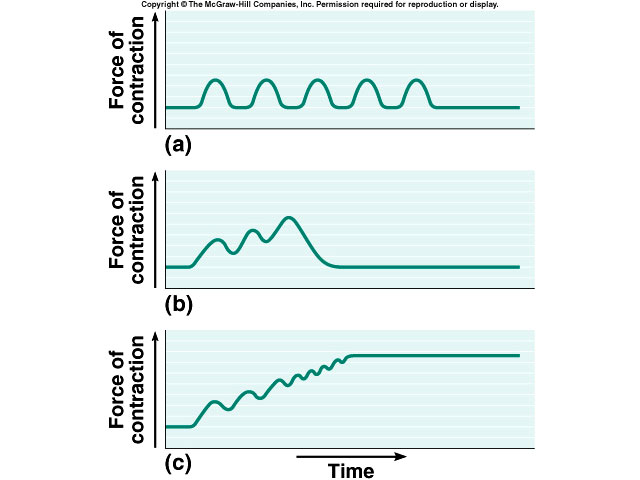
Wave summation is defined as if two stimuli are applied and the second one is delayed until the refractory period is over, the skeletal muscle will respond to both and the second will be stronger than the first. Tetanus can be partial or complete depending on the number of stimulations per second; most voluntary contractions involve short term tetanic contractions. The Staircase Effect (Treppe) is similar to wave summation, except there is complete relaxation between stimuli.
Number of Muscle Fibers Contracting
Recruitment is the process of increasing the number of active motor
units.
Muscle tone is the involuntary activation of a small number of motor units that causes sustained, small contractions that give firmness to a relaxed skeletal muscle. It is Essential for maintaining posture and keeping the head upright.
The different types of contractions are Isotonic where the muscle shortens during contraction, Isometric contraction where the muscle contracts but does not shorten, and Eccentric or Isokinetic contraction where the muscle lengthens.
TYPES OF MUSCLE TISSUE
|
|
Skeletal |
Smooth |
Cardiac |
|
Location |
Skeletal muscles |
Walls of hollow organs |
Wall of heart |
|
Function |
Movement of bones at joints |
Peristalsis |
Pumping action of heart |
|
Striations |
Present |
Absent |
Present |
|
Nucleus |
Multiple |
Single |
Single |
|
Mode of control |
Voluntary |
Involuntary |
Involuntary |
|
Contraction/ |
Relatively rapid |
Slowly, rhythmic |
Rhythmic |